
The sting of death all around him had Roger in grief and anxious about how he would cope should he contract COVID-19.
Watching some of his fellow dialysis patients’ come down with the disease and never return from hospital made him fearful. But fear and anxiety were not enough to make him take the jab.
Roger Briggs says he would rather die from COVID-19 than take the vaccines. Already battling diabetes, hypertension and chronic kidney disease, he was ready to take on the virus.
Driven by fears over the rapid development of the vaccines, he does not trust that they were tested sufficiently, and believes there isn’t sufficient data or science to ensure their safety.
A husband and father of four children and eight grandchildren, Roger will not take the vaccine that could protect his life.
“To what end?” he asks. “There are people who took the vaccine and didn’t do well. It may have been in the minority, but the vaccines are not working like vaccines should … “we all have to die.”
Every Monday, Wednesday and Friday, Roger makes his way to the John Hayes Memorial Kidney Foundation (JHMKF) in Belmont on the outskirts of the city of Port of Spain for his four-hour treatment.
Because of declining health, Roger hires a taxi to transport him to and from dialysis, and the transportation cost and money for medication sometimes, are steadily biting into his meagre savings.
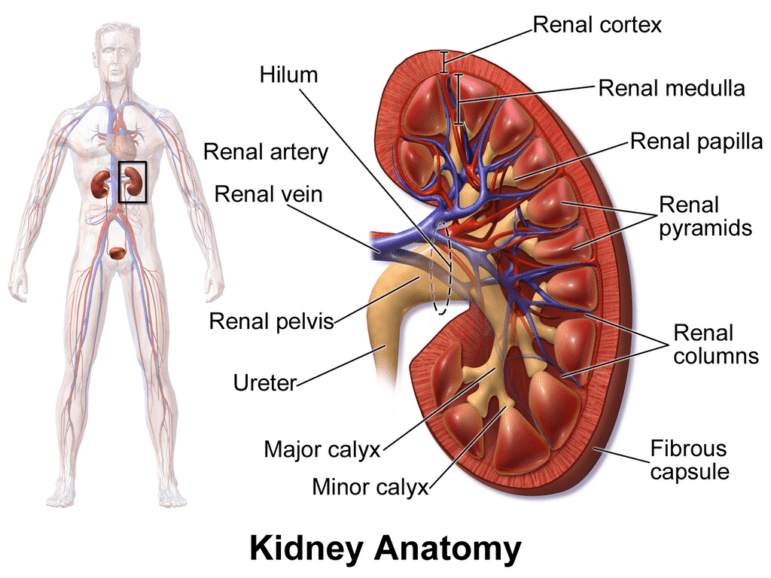
End stage renal disease or chronic kidney disease (CKD) is a debilitating illness that requires lifesaving treatments such as dialysis or a difficult to obtain organ transplant.
While dialysis offers people with CKD a lifeline, it too has its related complications such as hypotensive episodes, infections, cardiac arrhythmias, bleeding, and seizures.
Dialysis patients are restricted from consuming most green leafy vegetables, most tropical fruits, are discouraged from having foods with preservatives, and limited in their protein intake.
They are put on rigid diets to control their potassium, sodium, and phosphorus levels (electrolytes) which, if not managed, can lead to further complications such as heart attacks, strokes or even death.
Patients are also limited to one litre of fluid daily to prevent drowning: A process where too much fluid in the lungs that can cause patients to die of fluid overload.
Most patients lose the ability to urinate and require dialysis to remove any excess fluid and toxins from their bodies.
Already dealing with these drastic adjustments to Roger’s life, the COVID-19 pandemic only exacerbated an already difficult situation.
The Coming of COVID
Trinidad and Tobago registered its first COVID-19 positive case on March 12, 2020, and by the 22nd, the government closed the country’s borders to minimise exposure. While 2020 was a relatively manageable year for the country, April 2021 saw an explosion in the number of positive cases and consequent deaths.
The John Hayes Memorial Kidney Foundation registered one COVID death for 2020. Despite his best efforts, Roger contracted COVID-19 in July 2022.
Even after contracting the virus, he saw no reason for vaccine protection. He said it’s curious that the African continent with one of the lowest vaccination rates also has one of the lowest death rates.
When asked if he had to choose between dying from COVID or taking the vaccine, he calmly replied “I would not take the vaccine”.
But he quickly pointed out that he’s not an anti-vaxxer. “Yes, I have taken vaccines and I would take other vaccines that have been tested and proven for at least five years”. “I’m just not taking the COVID vaccine”, he stated emphatically.
He even praised the government saying he was impressed with how it handled the pandemic until it started saying it’s us against them.
“There should be freedom of choice and people should not be bullied into taking a vaccine”.

Roger is just one of forty-eight patients at the JHMKF who is hesitant to get vaccinated.
John Hayes’ longest living dialysis patient Heather Felix said she was conflicted. This year marks 23 years she’s been on dialysis, and she believes she is doing well.
“When the pandemic started, I panicked and I was going to take the vaccine, but I was between two minds.”
“Then you keep hearing about all these side effects and blood clots, so I decided not to take it.”
Heather said after weighing her options, she is not willing to risk taking the vaccine and possibly end up with further complications.
As nursing supervisor (JHMKF) Keston George explained, there is significant hesitancy at the centre.
“We did our best to explain why it was important to get vaccinated, but there was a bit of confusion amongst the renal population as to where they got their information from, and how they processed that information.”
“They were getting information from the Ministry of Health, social media and when they have discussions amongst themselves.”
He said there was a battle between what was factual and non-factual as well as how to decide who to trust, especially when even a few policy makers were questioning the legitimacy of the vaccines.
Such utterances, he said, had patients questioning the credibility of the vaccines and how quickly they were developed and tested.
One dialysis nurse with over 15 years’ experience said she would never take the vaccines, nor does she support giving them to dialysis patients.
“Why aren’t we having the same amount of deaths now?” she asked. “The death toll was fairly low until we started vaccinating the population and the minute we stopped, the death toll dropped.”
Nurse John, (not her real name) said dialysis patients didn’t fare any worse than those in the general population.
“The only difference with dialysis patients is they are more susceptible because they’re immuno-compromised.”
She was also displeased by the Ministry of Health’s statements that this was a “pandemic of the unvaccinated.”
“Remember when they were threatening healthcare workers that if they didn’t take the vaccines they would not be able to go to work?”
“So, these vaccines were being used for economic reasons.”
“Vaccinate to Operate”, she says, “was being pushed by the ministry (of health) and businesses who were more interested in reopening the economy than in the lives of their workers.”
Nurse John was asked, “If you had to choose between dying from the COVID virus and taking the vaccine, what would you choose?”
“I would choose death, but I don’t think I would have died.”
“These vaccines were only approved for emergency use and the developers aren’t willing to take any kind of responsibility for adverse effects. Hundreds of medical doctors advised people not to take the vaccines stating they are unsafe, and nobody knew what the long-term effects of the vaccines would be,” she stated emphatically.
“And whether you died from COVID or not, they were labelling it a COVID death,” she said.
The Classification of COVID Positive Deaths
Before the pandemic, JHMKF had 136 patients. That number was reduced to 90 at the start of 2023. JHMKF shared that 81 patients contracted the virus and 35 of them died – most of them elderly patients with comorbidities. The majority were unvaccinated.
However, there is the suggestion that the vaccination rate appeared to play little to no role as the death rate remained the same as before COVID-19.
A possible explanation for the anomaly was the widespread disagreement in the population about how COVID deaths were being classified.
Chief Medical Officer Dr Roshan Parasram said, “Anyone that passed away and has a COVID positive test at the time of death will be classified as dying with COVID.” As long as a patient was COVID positive at the time of death, he/she would be counted as a COVID death.
That proclamation raised ire amongst trade union leaders who believed that without a clear case definition for a COVID-19 fatality, the government could embellish the COVID deaths.
In addition to labelling all patients who died COVID positive as a COVID death, the Ministry of Health also issued guidelines and recommendations for hospital staff and funeral agencies in the handling of COVID positive bodies. As such, funeral homes were not allowed to perform postmortems or autopsies on anyone who died COVID positive.The Ministry of Health’s recommendation 5 (iii), stated “positive Covid-19 cases will not have an autopsy performed”.
These stipulations led to further disagreements with various religious groups about their burial rites.
The Data
At the onset of the pandemic, the US Centers for Disease Control (CDC), World Health Organisation (WHO) and and T&T’s Ministry of Health suggested that 95% of people who contract COVID will get a mild to moderate version of the virus and would not require hospitalisation.
COVID-19 deaths are calculated by the Case Fatality Rate (CFR). CFR is calculated by dividing the number of deaths from a specified disease over a defined period of time, by the number of individuals diagnosed with the disease during that time. The resulting ratio is then multiplied by 100 to yield a percentage.
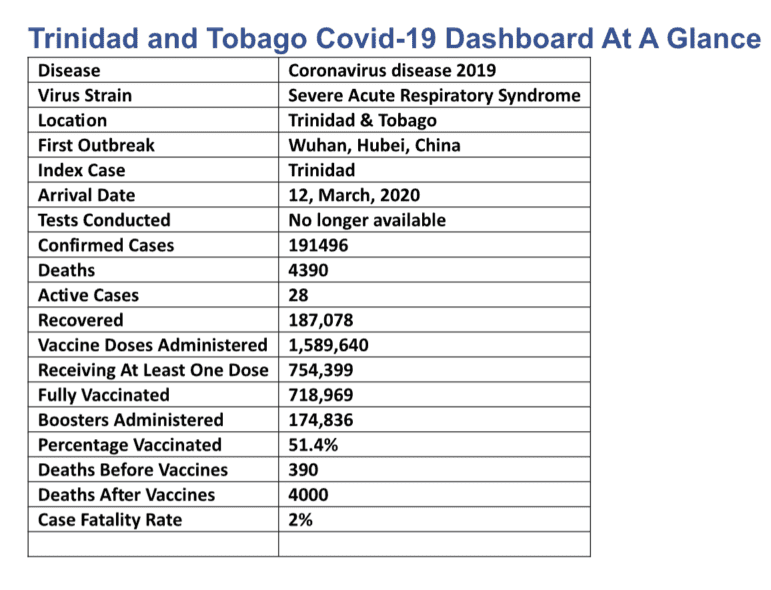
The online website Worldometer (worldometers.info) recorded 191,496 COVID positive cases as at June 19, and 4390 deaths.
CFR = 4390 ÷ 191496 = 0.02 x 100 = 2%. The case fatality rate for Trinidad and Tobago from the COVID-19 virus is two percent (2%).
CFR = 35 ÷ 81 = .43 X 100 = 43%. The case fatality rate for JHMKF is forty-three percent (43%).
JHMKF CFR before the pandemic was approximately 30%.
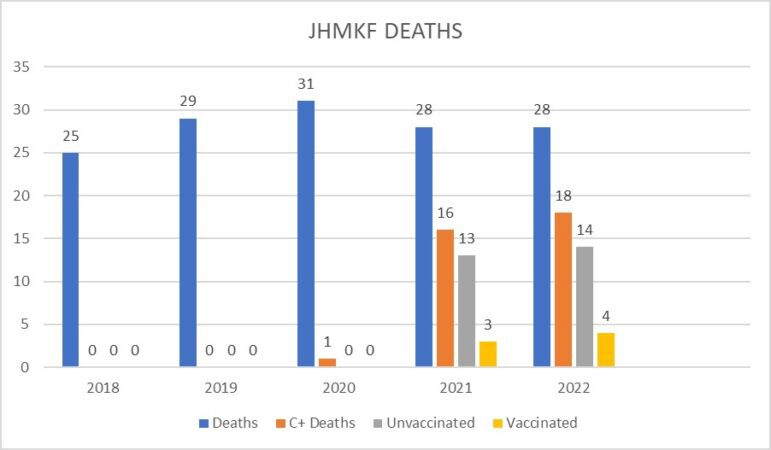
The data shows that before the pandemic, deaths at JHMKF averaged 27 per year and that jumped to 29 per year with the pandemic. The data shows that patients were not dying at a faster rate since the onset of COVID, and those who tested COVID positive and died did not die from the virus but from their underlying comorbidities.
The Ministry of Health’s COVID-19 update shows that before the vaccine rollout, there were 390 deaths. Since the vaccines were introduced, 3665 patients who were not fully vaccinated and 335 fully vaccinated patients died. These figures suggest that ten times more people died after the introduction of the vaccines.
Despite its daily press briefings, social media campaigns, interviews and media blitz, the Ministry of Health was unable to get more than half of the population vaccinated.
After three years of the pandemic, only 51.4% of the population is fully vaccinated.
To date, there is limited data available to determine the rate of hesitancy with dialysis patients throughout the country.
Nephrologist Dr Steven Goorachan said there are 1200 dialysis patients and the COVID death rate is approximately 28%. But without data from the Ministry of Health to show how many patients contracted COVID, it’s impossible to calculate the CFR in the dialysis population.
Interview and data requests sent to the Ministry of Health since March 21 have yielded no result to date.
Communications Consultant at the ministry, Shemelle Paradice, said while the ministry is willing to provide the data, it takes time to put it together and there are concerns about breaches of patient confidentiality.
When it was pointed out that the Ministry was sharing similar data during their daily press briefings, the correspondence went cold.
Similarly, Dr Erica Wheeler who heads the PAHO office in Port of Spai said she would be happy to help but had to forward our request to Washington DC to source the relevant data. Follow up emails requesting feedback remain unanswered.
Vaccine Support
While some patients were hesitant to take the vaccines, doctors fully supported being vaccinated against COVID-19. In an interview with Media Institute of the Caribbean (MIC), Nephrologists Boris Mohammed and Steven Goorachan agreed that hesitancy was only one of the issues plaguing dialysis patients.
They said dialysis patients died at a rate comparable to worldwide figures https://pubmed.ncbi.nlm.nih.gov/35381932/, but believe some of these deaths could have been avoided.
They said the healthcare system’s slow response to getting COVID positive patients dialysed, led to unnecessary deaths.
“You weren’t allowed to be dialysed at your center because you had to be in isolation and that means you missed sessions. And once you miss sessions, you could die!”
“Patients who were on dialysis were not able to get dialysis in a timely manner, and that’s what contributed to their high death rate”. exclaimed Dr Mohammed.
Dr Goorachan shared the sentiment. “I think we had other factors but as Dr Mohammed alluded to, was actually being able to seek dialysis therapies and be COVID positive initially, I think that’s what contributed to our higher outcomes”.
Apart from the slow response, Dr Goorachan said the dialysis population is an at-risk population. As ProPublica reports, dialysis patients were the pandemic’s perfect victims.
Dr Goorachan also pointed out that the hesitancy was driven by how quickly the vaccines were developed. He said patients did not trust the new technology.
However, both doctors agreed the risks of the disease outweigh the risks of the vaccines. Dr Mohammed admitted he was initially afraid to get vaccinated, but he would rather take his chances with the vaccines than the virus.
Dr Goorachan said if you examined the benefits of the vaccines, they offer far greater protection than any side effects, and to expect a vaccine to have no side effects is unrealistic.
Weighing in on the importance of the vaccines is immunologist and lecturer at the University of the West Indies Dr Carla Maria Alexander who said the vaccines are safe for dialysis patients.
She said while patients are immuno-suppressed or immuno-compromised, that’s no reason not to be vaccinated.
Dr Alexander admitted that the vaccines would not offer the same level of protection to dialysis patients due to their weakened immune systems, but the booster shots would provide the additional protection required. See the question-and-answer segment with Dr Alexander here.
Back at JHMKF, there were also patients who supported taking the jab. Nicolan Bushell took most of her information from the Ministry of Health and got herself and her daughter vaccinated as soon as vaccines became available.
She laughingly admitted that she decided on the Sinopharm vaccine because if the virus was from Wuhan China, then certainly the best vaccine would also be from China.
‘It sounds stupid even listening to myself saying it now, but that’s what was going through my mind at the time”, she stated frankly.
And as much as she believes in the safety of the vaccines, she admitted her daughter have been questioning the adverse effects of the vaccines, as she’s been experiencing changes in her body that she attributes to the vaccine. Listen to the full interview here:
Also in support of the vaccines are the dialysis patients at the IME (Institute of Medical Education) Dialysis Center in southern Trinidad. Sixty-five percent (65%) of them took the vaccines understanding they would be protected from the virus, but the others refused.
Manager at IME, Patricia Clarke said those patients believed the vaccines would only compound their kidney issues.
“They don’t believe the risk is worth it. They saw a lot of people who were vaccinated got severely ill and even died”.
“As much as you want them to get vaccinated, you can’t argue with their beliefs that their kidneys are already compromised and might not be able to mount an adequate response to the virus”.Twelve of the 76 patients at IME contracted the virus but none of them died from the virus. Seven were vaccinated and five unvaccinated. IME’s Case Fatality Rate is zero.
Dialysis patients such as Roger and Heather, along with a number of health care providers who work to protect them, believe the pandemic raised numerous questions. To them, some grey areas, including the vaccine concerns associated with dialysis treatment, remain unanswered – whatever the officials say.
This reporting was supported by the International Women’s Media Foundation’s Global Health Reporting Initiative: Vaccines and Immunization in the Caribbean, in partnership with Sabin Vaccine Institute.